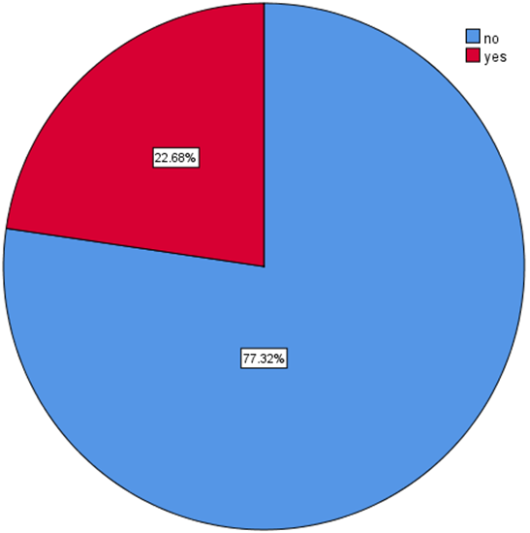
Introduction: - Birth trauma, often known as birth injuries, is any disability or harm that a newborn sustains during delivery or throughout the entire birth process. According to Ethiopia, birth injuries now contribute to between 28% and 31.6% of neonatal deaths, making them the major cause of mortality and morbidity. Although research on the extent and risk factors was conducted in Ethiopia, it did not cover all aspects, such as medical factors (smoking) and professional factors that were proven to be predictors of birth injury in other nations. Methods: An institutional-based cross-sectional study was employed for three months from June 1, 2023, to August 30, 2023. A semi-structured interview-administered questionnaire was used to collect data. Data were entered into Epi Data version 4.6 and exported to Statistical Package for Social Science software version 26 for analysis. Descriptive statistical analysis was done, and an association between dependent variables and independent variables was examined in logistic regression models. Results: The overall magnitude of neonatal birth injuries was 22.68% (95% CI: 18.5, 27.5). Age of the mother from 15-19 and 20-24 (AOR: 0.006, 95% CI:0.000, 0.131, and AOR: 0.017, 95% CI:0.001, 0.320), instrumental delivery (AOR:3.882, 95% CI:1.402, 10.780), cesarean section (AOR: 0.1449, 95% CI:0.027, 0.779), rural residence (AOR: 3.188, 95% CI:1.283, 7.923), cephalo-pelvic disproportion (AOR: 8.171, 95% CI:3.871, 17.248), induced labor (AOR: 4.009, 95% CI:1.832, 8.773), and prolonged duration of labor (AOR: 5.262, 95% CI:2.222, 12.461) were risk factors of birth injury. Conclusion and Recommendation: The rate of birth injuries was found to be higher than expected. The age of the mother, instrumental and cesarean section delivery, prolonged labor, induced labor, CPD, and rural residence were predictors of birth injury. The Ministry of Health and the regional and local healthcare systems should give attention to maternal health services.
| Published in | Biomedical Statistics and Informatics (Volume 10, Issue 1) |
| DOI | 10.11648/j.bsi.20251001.11 |
| Page(s) | 1-13 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Birth Injury, Fiche, North Shewa, Oromia
Variables | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
Age of the mother | 15-19 | 33 | 10.5 |
20-24 | 80 | 25.6 | |
25-29 | 105 | 33.5 | |
30-34 | 58 | 18.5 | |
≥35 | 37 | 11.8 | |
Level of education | No Formal education | 86 | 27.5 |
Primary | 73 | 23.3 | |
Secondary | 94 | 30.0 | |
More than secondary | 60 | 19.2 | |
Residence | Urban | 201 | 64.2 |
Rural | 112 | 35.8 | |
Marital status | Single | 13 | 4.2 |
Married | 289 | 92.3 | |
Divorced | 11 | 3.5 | |
Pre-pregnancy weight/BMI (Kg/m2) | <18.5 | 42 | 13.4 |
18.5-24.9 | 237 | 75.7 | |
25-29.9 | 31 | 9.9 | |
≥30 | 3 | 1.0 | |
Height of the mother in cm | <145 cm | 34 | 10.9 |
≥145 cm | 279 | 89.1 |
Variables | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
Having a history of ANC | Yes | 296 | 94.6 |
No | 17 | 5.4 | |
Visited health services for ANC | <4 follow-up | 74 | 23.6 |
4 and above | 222 | 70.9 | |
No follow up | 17 | 5.5 | |
Facilities for ANC | Health center | 88 | 28.1 |
Governmental hospital | 208 | 66.5 | |
Parity | Primipara | 109 | 34.8 |
Multipara | 204 | 65.2 | |
Gravidity | Primigravida | 109 | 34.8 |
Multigravida | 204 | 65.2 | |
Pregnancy-induced hypertension | Yes | 17 | 5.4 |
No | 296 | 94.6 | |
Smoking cigarette | Yes | 7 | 2.2 |
No | 306 | 97.8 | |
Type of pregnancy | Single | 286 | 91.4 |
Twine | 27 | 8.6 | |
Vaginal bleeding during pregnancy | Yes | 44 | 14.1 |
No | 269 | 85.9 |
Variables | Category | Birth injury | |
|---|---|---|---|
No | Yes | ||
Fetal presentation | Vertex presentation | 204(79.4%) | 53(20.6%) |
Breech presentation | 18(75%) | 53(25%) | |
Face presentation | 12(85.7%) | 2(14.3%) | |
Brow presentation | 8(50%) | 8(50%) | |
Shoulder presentation | 0 | 2(100%) | |
Cephalo-pelvic disproportion | No | 210(87.1%) | 31(12.9%) |
Yes | 32(44.4%) | 40(55.6%) | |
Did labor start at term? | No | 28(84.8%) | 5(15.2%) |
Yes | 214(76.4%) | 66(23.6%) | |
Conditions of labor | Spontaneous | 195(86.7%) | 30(13.7%) |
Induced | 36(46.8%) | 56(48.3%) | |
Duration of labor | >12hr(prolonged) | 60(51.7%) | 56(48.3%) |
<12hr(non-prolonged) | 171(91.9%) | 15(8.1%) | |
Mode of delivery | Spontaneous vaginal delivery | 180(90.5%) | 19(8.1%) |
Instrumental delivery | 45(49.5%) | 46(50.5%) | |
Cesarean section | 17(73.9%) | 6(26.1%) | |
Time of birth | Day time birth | 146(75.6%) | 47(24.4%) |
Night time birth | 96(80%) | 24(20%) | |
Variables | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
Sex | Male | 220 | 70.3 |
Female | 93 | 29.7 | |
Gestational age | <37wk | 42 | 13.4 |
37wk-42wk | 271 | 86.6 | |
Weight | <2500 gram | 54 | 17.3 |
2500-3999 gram | 249 | 79.6 | |
≥4000 gram | 10 | 3.2 | |
Head circumference | <33 cm | 23 | 7.3 |
33-38 cm | 278 | 88.8 | |
>38 cm | 12 | 3.2 |
Variable | Category | Birth injury | |
|---|---|---|---|
No | Yes | ||
Qualification of birth attendant | Gynecologist | 14(43.8%) | 18(56.3%) |
General practitioner | 8(44.4%) | 10(55.6%) | |
Midwifery | 197(88.7%) | 25(11.3%) | |
IESO | 23(56.1%) | 18(43.9%) | |
Year of experience | <3 | 63(67.7%) | 30(32.3%) |
4-5 | 133(82.6%) | 28(17.4%) | |
≥6 | 46(78%) | 13(22%) | |
Given special training | No | 83(76.1%) | 26(23.9%) |
Yes | 159(77.9%) | 45(22.1%) | |
Fully availability of delivery materials | No | 44(78.6%) | 12(21.4%) |
Yes | 198(77%) | 59(23%) | |
Availability of different guidelines | No | 21(91.3%) | 2(8.7%) |
Yes | 221(76.2%) | 69(23.8) | |
Parthograph utilization | No | 11(84.6%) | 2(15.4%) |
Yes | 230(76.9%) | 69(23.1%) | |
Variables | Category | Birth injury | COR (95%CI) | AOR (95%CI) | P value | |
|---|---|---|---|---|---|---|
Yes | No | |||||
Age of the mother | 15-19 | 11 | 22 | 0.222((0.079-0.621) | 0.006(0.000-0.131)* | 0.001 |
20-24 | 8 | 72 | 0.561(0.238-0.964) | 0.017(0.001-0.320)* | 0.000 | |
≥35 | 11 | 26 | 1 | 1 | 1 | |
Fetal presentation | Vertex presentation | 53 | 204 | 1 | 1 | 1 |
Breech presentation | 6 | 18 | 1.283(0.485-3.392) | 2.004(0.515-7.795) | 0.316 | |
Face presentation | 2 | 12 | 0.642(0.139-2.954) | 0.255(0.027-2.455) | 0.237 | |
Brow presentation | 8 | 8 | 3.849(1.380-10.773) | 0.513(0.124-4.016) | 0.567 | |
Qualification of birth attendant | Gynecologist | 18 | 14 | 1 | 1 | 1 |
General practitioner | 10 | 8 | 0.972(0.304-3.110) | 0.229(0.035-1.500) | 0.124 | |
Midwifery | 25 | 197 | 0.99(0.044-0.223) | 2.380(0.396-14.302) | 0.343 | |
IESO | 18 | 23 | 0.609(0.240-1.546) | 0.462(0.137-1.556) | 0.213 | |
Pre-pregnancy weight/BMI | <18.5 | 12 | 30 | 1 | 1 | 1 |
18.5-24.9 | 44 | 193 | 0.570(0.271-1.201) | 0.511(0.172-1.517) | 0.227 | |
25-29.9 | 12 | 19 | 1.579(0.590-4.229) | 2.501(0.659-9.493) | 0.178 | |
Year of professional experience | <3 | 30 | 63 | 1 | 1 | 1 |
4-5 | 28 | 133 | 0.442(0.244-0.802) | 1.462(0.388-5.506) | 0.575 | |
>6 | 13 | 46 | 0.593(0.279-1.2610 | 0.489(0.144-1.661) | 0.251 | |
Marital status | Single | 2 | 11 | 1 | 1 | 1 |
Married | 64 | 225 | 1.564(0.338-7.239) | 3.388(0.392-29.299) | 0.268 | |
Divorced | 5 | 6 | 4.583(0.673-31.198) | 7.842(0.542-113.560) | 0.131 | |
Head circumference | <33 cm | 4 | 19 | 1 | 1 | 1 |
33-38 cm | 55 | 233 | 1.172(0.383-3.583) | 0.355(0.072-1.751) | 0.203 | |
Mode of delivery | Normal vaginal delivery | 19 | 180 | 1 | 1 | 1 |
Instrumental delivery | 46 | 45 | 9.684(5.176-18.118) | 3.882(1.402-10.780)* | 0.009 | |
Cesarean section | 6 | 17 | 3.344(1.177-9.497) | 0.1449(0.027-0.779)* | 0.024 | |
Weight | <2500 gram | 8 | 46 | 1 | 1 | 1 |
2500-3999 gram | 53 | 196 | 1.555(0.692-3.494) | 2.469(0.776-7.849) | 0.126 | |
Residence | Urban | 36 | 165 | 1 | 1 | 1 |
Rural | 35 | 77 | 2.083(1.216-3.569) | 3.188(1.283-7.923)* | 0.013 | |
Height | <145 cm | 14 | 20 | 1 | 1 | 1 |
≥145 cm | 57 | 222 | 0.367(0.175-0.771) | 0.615(0.130-2.915) | 0.540 | |
Pregnancy-induced hypertension | Yes | 7 | 10 | 0.394(0.144-1.076) | 0.445(0.050-3.982) | 0.469 |
No | 64 | 232 | 1 | 1 | 1 | |
Cephalo-pelvic disproportion | Yes | 40 | 31 | 8.468(4.654-15.407) | 8.171(3.871-17.248)* | 0.000 |
No | 31 | 211 | 1 | 1 | 1 | |
Conditions of labor | Spontaneous | 30 | 195 | 1 | 1 | 1 |
Induced | 41 | 36 | 7.403(4.103-13.355) | 4.009(1.832-8.773)* | 0.001 | |
Gestational age | <37wk | 6 | 36 | 1 | 1 | 1 |
37wk-42wk | 65 | 206 | 0.528(0.213-1.310) | 0.301(0.042-2.151) | 0.231 | |
Baby sex | Male | 58 | 162 | 0.454(0.235-0.877) | 0.562(0.195-1.621) | 0.287 |
Female | 13 | 80 | 1 | 1 | 1 | |
Availability of different guidelines | Yes | 69 | 221 | 0.305(0.070-1.334) | 0.021(0.000-2.961) | 0.126 |
No | 2 | 21 | 1 | 1 | 1 | |
Duration of labor in hours | >12hr(prolonged) | 56 | 60 | 10.640(5.603-20.204) | 5.262(2.222-12.461)* | 0.000 |
<12hr(non-prolonged) | 15 | 171 | 1 | 1 | 1 | |
AOR | Adjusted Odd Ratio |
ANC | Antenatal Care |
BMI | Body Mass Index |
BT | Birth Trauma |
CI | Confident Interval |
CPD | Cephalo-pelvic Disproportion |
C/S | Caesarian Section |
CDC | Centers for Disease Control |
COR | Crude Odd Ratio |
IESO | Integrated Emergency Surgical Officers |
IRB | Institutional Review Board |
NGO | Non- Governmental Organization |
PI | Principal Investigator |
| [1] | MCEE W. MCEE-WHO methods and data sources for child causes of death 2000–2015. World Health Organization. 2016. |
| [2] | Tibebu EA, Desta KW, Ashagre FM, Jemberu AA. Prevalence of birth injuries and associated factors among newborns delivered in public hospitals Addis Ababa, Ethiopia, 2021. Crossectional study. Plos one. 2023; 18(1): e0281066. |
| [3] | Belay AS, Negese K, Manaye GA, Debebe S. Prevalence and associated factors of birth injury among neonates admitted at neonatal intensive care unit (NICU) in governmental hospitals of Southwest Ethiopian people regional state, Ethiopia: A multicentric cross-sectional study. Frontiers in Pediatrics. 2022; 10. |
| [4] | Basiri B, Solgi MS, Sabzehi MK, Eghbalian F, Nasrolahi S, Jiriaee N, et al. Prevalence of Birth Injury and Its Determinants Factors in West Iran in 2020-2021. Medical-Surgical Nursing Journal. 2022; 11(3). |
| [5] | Jeergal NA, Thobbi A, Katti SV. A clinical study of neonatal birth injuries in a tertiary care hospital-NICU, Bijapur. Indian Journal of Child Health. 2020; 7(7): 288-90. |
| [6] | Pius S, Ibrahim H, Ibrahim B, Farouk A, Machoko Y, Bello M. Incidence and characteristics of neonatal birth injuries in Maiduguri North-Eastern Nigeria. Nigerian Journal of Paediatrics. 2018; 45(2): 99-105. |
| [7] | Iacoella F, Tirivayi N. Determinants of maternal healthcare utilization among married adolescents: Evidence from 13 Sub-Saharan African countries. Public Health. 2019; 177: 1-9. |
| [8] | El Beltagy MA, Elbaroody M. The diagnosis and management of abusive head injuries in infancy in Egypt. Child's nervous system. 2023: 1-5. |
| [9] | Buxton H, Flynn E, Oluyinka O, Cumming O, Esteves Mills J, Shiras T, et al. Hygiene during childbirth: an observational study to understand infection risk in healthcare facilities in Kogi and Ebonyi states, Nigeria. International journal of environmental research and public health. 2019; 16(7): 1301. |
| [10] | Mulugeta T, Sebsibe G, Fenta FA, Sibhat M. Risk factors of perinatal asphyxia among newborns delivered at public hospitals in Addis Ababa, Ethiopia: a case-control study. Pediatric health, medicine, and therapeutics. 2020: 297-306. |
| [11] | Abdo RA, Halil HM, Kebede BA, Anshebo AA, Gejo NG. Prevalence and contributing factors of birth asphyxia among the neonates delivered at Nigist Eleni Mohammed Memorial Teaching Hospital, Southern Ethiopia: a cross-sectional study. BMC pregnancy and childbirth. 2019; 19: 1-7. |
| [12] | Belay AS, Achimano AA. Prevalence and Risk Factors for Periodontal Disease Among Women Attending Antenatal Care in Public Hospitals, Southwest Ethiopia, 2022: A Multicenter Cross-Sectional Study. Clinical, Cosmetic, and Investigational Dentistry. 2022; 14: 153-70. |
| [13] | Leinweber J, Fontein‐Kuipers Y, Thomson G, Karlsdottir SI, Nilsson C, Ekström‐Bergström A, et al. Developing a woman‐centered, inclusive definition of traumatic childbirth experiences: A discussion paper. Birth. 2022; 49(4): 687-96. |
| [14] | Nagle U, Naughton S, Ayers S, Cooley S, Duffy RM, Dikmen-Yildiz P. A survey of perceived traumatic birth experiences in an Irish maternity sample–prevalence, risk factors and follow up. Midwifery. 2022; 113: 103419. |
| [15] | Mundorf A, Bölükbas I, Freund N. Maternal separation: Does it hold the potential to model consequences of postpartum depression? Developmental Psychobiology. 2022; 64(1): e22219. |
| [16] | Kaijomaa M, Gissler M, Äyräs O, Sten A, Grahn P. Impact of simulation training on the management of shoulder dystocia and incidence of permanent brachial plexus birth injury: An observational study. BJOG: An International Journal of Obstetrics & Gynaecology. 2023. |
| [17] | Paran TS, Puri P. Birth Trauma. Pediatric Surgery: Diagnosis and Management: Springer; 2023. p. 219-28. |
| [18] | Sagan ML, Juan AS. Birth Fractures. Orthopedics for the Newborn and Young Child: A Practical Clinical Guide: Springer; 2023. p. 199-208. |
| [19] | Biset G, Mihret S, Mekonen AM, Workie A. Magnitude of birth trauma and its associated factors in South Wollo public hospitals, northeast Ethiopia, August 2021: Institutional-Based Cross-Sectional Study. BMJ open. 2022; 12(9): e057567. |
| [20] | Tesfaye W, Workneh N, Girma E. Birth injury and associated factors in Jimma University Specialized Hospital, southwest Ethiopia. Ethiopian Journal of Pediatrics and Child Health. 2017; 12(1). |
| [21] | Yemane A, Yeshidinber A. Birth trauma among neonates admitted to the neonatal unit in a tertiary hospital in Addis Ababa. Ethiopian Journal of Pediatrics and Child Health. 2019; 14(1). |
| [22] | Abadiga M, Mosisa G, Tsegaye R, Oluma A, Abdisa E, Bekele T. Determinants of adverse birth outcomes among women delivered in public hospitals of Ethiopia, 2020. Archives of Public Health. 2022; 80(1): 1-17. |
| [23] | Palo SK, Dubey S, Negi S, Sahay MR, Patel K, Swain S, et al. Effective interventions to ensure MCH (maternal and child health) services during pandemic-related health emergencies (Zika, Ebola, and COVID-19): a systematic review. PLoS One. 2022; 17(5): e0268106. |
| [24] | Acharya K, Subedi D, Acharya P. Health facility readiness to provide integrated Family Planning, Maternal and Child Health (FPMCH) services in Nepal: Evidence from the comprehensive health facility survey. Plos one. 2022; 17(2): e0264417. |
| [25] | Goyomsa G, Deriba B, Wadejo M, Debela S. Magnitude of Neonatal Near Miss and Associated factors among Newborn delivered at North Shewa Zone Public Health Hospital, Central Ethiopia: Multi-level analysis. Frontiers in Public Health. 2022: 3482. |
| [26] | Georges Pius K, Aurore Albane E, Marie-Paul B, Komba D, Ngando V, Eteme A. Neonatal Sepsis: Highlights and Controversies. J Pediatr Neonatal. 2022; 4(1): 1-5. |
| [27] | Ami O, Maran J-C, Cohen A, Hendler I, Zabukovek E, Boyer L. Childbirth simulation to assess cephalopelvic disproportion and chances for failed labor in a French population. Scientific Reports. 2023; 13(1): 1110. |
| [28] | Darma IY, Abdillah N, editors. THE EFFECT OF THE IMPLEMENTATION ACTIVE BIRTH TECHNIQUE USING A BIRTH BALL AND HYPNOBIRTHING ACCELERATED THE PROGRESS OF THE FIRST STAGE OF LABOR AMONG INTRAPARTUM MOTHERS. Proceeding International Conference Syedza Saintika; 2020. |
| [29] | Ahmed E. Obstructed Labor and its Associated Factors Among Mothers Who Gave Birth at Public Hospitals, in South Gondar Zone, North West Ethiopia Principal investigator 2022. |
| [30] | Osinaike B, Akinseye L, Akiyode O, Anyaebunam C, Kushimo O. Prevalence and predictive factors of birth traumas in neonates presenting to the children emergency center of a tertiary center in Southwest, Nigeria. Journal of Clinical Sciences. 2017; 14(4): 167-. |
| [31] | Warke C, Malik S, Chokhandre M, Saboo A. Birth injuries-A review of incidence, perinatal risk factors and outcome. Bombay Hosp J. 2012; 54(2): 202-8. |
| [32] | Abedzadeh-Kalahroudi M, Talebian A, Jahangiri M, Mesdaghinia E, Mohammadzadeh M. Incidence of neonatal birth injuries and related factors in Kashan, Iran. Archives of trauma research. 2015; 4(1). |
| [33] | Abdollahpour S, Khadivzadeh T. Prevalence of traumatic childbirth and post-traumatic stress after delivery in Iran: a systematic review and meta-analysis. Journal of Obstetrics, Gynecology and Cancer Research. 2022; 4(3): 86-92. |
| [34] | Ray S, Mondal R, Samanta M, Hazra A, Sabui TK, Debnath A, et al. Prospective study of neonatal birth trauma: Indian perspective. Journal of Clinical Neonatology. 2016; 5(2): 91-5. |
| [35] | Christensen TR, Bahr TM, Henry E, Ling CY, Hanton TH, Page JM, et al. Neonatal sub-galeal hemorrhage: twenty years of trends in incidence, associations, and outcomes. Journal of Perinatology. 2023; 43(5): 573-7. |
| [36] | Salgado HdO, Queiroz MR, Dos Santos HG, Andreucci CB, Diniz CSG. Using the Maternity Safety Thermometer to estimate harm‐free care in Southeast Brazil: A hospital‐based cohort. Birth. 2019; 46(4): 583-91. |
| [37] | Uchenna E, Chidiebere OD, Nwabueze AI. Birth injuries in the newborn: a prospective study of deliveries in South-East Nigeria. African Journal of Medical and Health Sciences. 2021; 20(4): 41-6. |
| [38] | Hollander M, de Miranda E, Smit A-M, de Graaf I, Vandenbussche F, van Dillen J, et al. ‘She convinced partner involvement in choosing a high-risk birth setting against medical advice in the Netherlands: A qualitative analysis. Plos one. 2020; 15(2): e0229069. |
| [39] | Prabhu RS, Sajjid M, Anandan H. Incidence and predisposing factors of birth trauma in a tertiary care hospital in Chennai, India: a prospective study. International journal of scientific study. 2017; 4(10): 29-33. |
| [40] | West BA, Okari T. Incidence, Pattern and Outcome of Birth Injuries as Seen in a Tertiary Hospital in Southern Nigeria. |
| [41] | Nanda S. Evaluation and Management of High-Risk Pregnancies: Emerging Research and Opportunities: Emerging Research and Opportunities. 2020. |
| [42] | Febrina E. HUBUNGAN TINGKAT ANEMIA PADA IBU HAMIL DENGAN ANGKA KEJADIAN RETENSIO PLASENTA: UNIMUS; 2017. |
| [43] | Neal S, Channon AA, Chintsanya J. The impact of young maternal age at birth on neonatal mortality: Evidence from 45 low and middle-income countries. PloS one. 2018; 13(5): e0195731. |
| [44] | Aminullah A, Budiwardhana N, Firmansyah A. Neonatal birth trauma: incidence and predisposing factors. Paediatrica Indonesiana. 2003; 43(6): 220-5. |
| [45] | Mah E, Foumane P, Ngwanou D, Nguefack S, Chiabi A, Dobit J, et al. Birth injuries in neonates at a university teaching hospital in Cameroon: epidemiological, clinical and therapeutic aspects. Open Journal of Pediatrics. 2017; 7(01): 51. |
APA Style
Alemu, T. T., Beyene, D. H., Zergaw, M. W., Mirkena, G. B., Delelegn, H. A. (2025). Magnitude of Birth Injuries and Associated Factors Among Newborns Delivered in Public Hospitals of North Shewa Zone, Oromia, Ethiopia, 2023: Cross-Sectional Study. Biomedical Statistics and Informatics, 10(1), 1-13. https://doi.org/10.11648/j.bsi.20251001.11
ACS Style
Alemu, T. T.; Beyene, D. H.; Zergaw, M. W.; Mirkena, G. B.; Delelegn, H. A. Magnitude of Birth Injuries and Associated Factors Among Newborns Delivered in Public Hospitals of North Shewa Zone, Oromia, Ethiopia, 2023: Cross-Sectional Study. Biomed. Stat. Inform. 2025, 10(1), 1-13. doi: 10.11648/j.bsi.20251001.11
AMA Style
Alemu TT, Beyene DH, Zergaw MW, Mirkena GB, Delelegn HA. Magnitude of Birth Injuries and Associated Factors Among Newborns Delivered in Public Hospitals of North Shewa Zone, Oromia, Ethiopia, 2023: Cross-Sectional Study. Biomed Stat Inform. 2025;10(1):1-13. doi: 10.11648/j.bsi.20251001.11
@article{10.11648/j.bsi.20251001.11,
author = {Teferi Tasew Alemu and Dejene Hailu Beyene and Melese Wagaye Zergaw and Gadisa Berhanu Mirkena and Henok Abebayehu Delelegn},
title = {Magnitude of Birth Injuries and Associated Factors Among Newborns Delivered in Public Hospitals of North Shewa Zone, Oromia, Ethiopia, 2023: Cross-Sectional Study
},
journal = {Biomedical Statistics and Informatics},
volume = {10},
number = {1},
pages = {1-13},
doi = {10.11648/j.bsi.20251001.11},
url = {https://doi.org/10.11648/j.bsi.20251001.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.bsi.20251001.11},
abstract = {Introduction: - Birth trauma, often known as birth injuries, is any disability or harm that a newborn sustains during delivery or throughout the entire birth process. According to Ethiopia, birth injuries now contribute to between 28% and 31.6% of neonatal deaths, making them the major cause of mortality and morbidity. Although research on the extent and risk factors was conducted in Ethiopia, it did not cover all aspects, such as medical factors (smoking) and professional factors that were proven to be predictors of birth injury in other nations. Methods: An institutional-based cross-sectional study was employed for three months from June 1, 2023, to August 30, 2023. A semi-structured interview-administered questionnaire was used to collect data. Data were entered into Epi Data version 4.6 and exported to Statistical Package for Social Science software version 26 for analysis. Descriptive statistical analysis was done, and an association between dependent variables and independent variables was examined in logistic regression models. Results: The overall magnitude of neonatal birth injuries was 22.68% (95% CI: 18.5, 27.5). Age of the mother from 15-19 and 20-24 (AOR: 0.006, 95% CI:0.000, 0.131, and AOR: 0.017, 95% CI:0.001, 0.320), instrumental delivery (AOR:3.882, 95% CI:1.402, 10.780), cesarean section (AOR: 0.1449, 95% CI:0.027, 0.779), rural residence (AOR: 3.188, 95% CI:1.283, 7.923), cephalo-pelvic disproportion (AOR: 8.171, 95% CI:3.871, 17.248), induced labor (AOR: 4.009, 95% CI:1.832, 8.773), and prolonged duration of labor (AOR: 5.262, 95% CI:2.222, 12.461) were risk factors of birth injury. Conclusion and Recommendation: The rate of birth injuries was found to be higher than expected. The age of the mother, instrumental and cesarean section delivery, prolonged labor, induced labor, CPD, and rural residence were predictors of birth injury. The Ministry of Health and the regional and local healthcare systems should give attention to maternal health services.
},
year = {2025}
}
TY - JOUR T1 - Magnitude of Birth Injuries and Associated Factors Among Newborns Delivered in Public Hospitals of North Shewa Zone, Oromia, Ethiopia, 2023: Cross-Sectional Study AU - Teferi Tasew Alemu AU - Dejene Hailu Beyene AU - Melese Wagaye Zergaw AU - Gadisa Berhanu Mirkena AU - Henok Abebayehu Delelegn Y1 - 2025/01/09 PY - 2025 N1 - https://doi.org/10.11648/j.bsi.20251001.11 DO - 10.11648/j.bsi.20251001.11 T2 - Biomedical Statistics and Informatics JF - Biomedical Statistics and Informatics JO - Biomedical Statistics and Informatics SP - 1 EP - 13 PB - Science Publishing Group SN - 2578-8728 UR - https://doi.org/10.11648/j.bsi.20251001.11 AB - Introduction: - Birth trauma, often known as birth injuries, is any disability or harm that a newborn sustains during delivery or throughout the entire birth process. According to Ethiopia, birth injuries now contribute to between 28% and 31.6% of neonatal deaths, making them the major cause of mortality and morbidity. Although research on the extent and risk factors was conducted in Ethiopia, it did not cover all aspects, such as medical factors (smoking) and professional factors that were proven to be predictors of birth injury in other nations. Methods: An institutional-based cross-sectional study was employed for three months from June 1, 2023, to August 30, 2023. A semi-structured interview-administered questionnaire was used to collect data. Data were entered into Epi Data version 4.6 and exported to Statistical Package for Social Science software version 26 for analysis. Descriptive statistical analysis was done, and an association between dependent variables and independent variables was examined in logistic regression models. Results: The overall magnitude of neonatal birth injuries was 22.68% (95% CI: 18.5, 27.5). Age of the mother from 15-19 and 20-24 (AOR: 0.006, 95% CI:0.000, 0.131, and AOR: 0.017, 95% CI:0.001, 0.320), instrumental delivery (AOR:3.882, 95% CI:1.402, 10.780), cesarean section (AOR: 0.1449, 95% CI:0.027, 0.779), rural residence (AOR: 3.188, 95% CI:1.283, 7.923), cephalo-pelvic disproportion (AOR: 8.171, 95% CI:3.871, 17.248), induced labor (AOR: 4.009, 95% CI:1.832, 8.773), and prolonged duration of labor (AOR: 5.262, 95% CI:2.222, 12.461) were risk factors of birth injury. Conclusion and Recommendation: The rate of birth injuries was found to be higher than expected. The age of the mother, instrumental and cesarean section delivery, prolonged labor, induced labor, CPD, and rural residence were predictors of birth injury. The Ministry of Health and the regional and local healthcare systems should give attention to maternal health services. VL - 10 IS - 1 ER -
Department of Nursing, Salale University Comprehensive Specialized Hospital, Fitche, Ethiopia