Background: This study aimed to identify the primary risk variables influencing the recurrence of cervical cancer in patients, at Tikur Anbessa Specialized Hospital. Cervical cancer deaths in Ethiopia reached 4,595, or 0.76% of total deaths. The age-adjusted death rate is 18.51 per 100,000 of the population in Ethiopia. Method: Among patients with cervical cancer, an institution-based retrospective follow-up research was conducted from January 2015 to March 2017 at TASH and is under follow-up. Out of a population of cervical cancer patients who were taking treatment in the hospital during that period, data on 420 patients is included in this study. Non-parametric methods, such as log-rank tests and the Kaplan-Meier method, were used to compare the rate of recurrence among the different explanatory variable categories. Results: After the medical cards of women were reviewed among those patients with cervical cancer, 170 (40.5%) were recurrent, and the remaining 250 (59.5%) were censored. Out of the total patients, 6.2% were at stage I, 32.6% were at stage II, 51.7% were at stage III, and 9.5% were at stage IV. The recurrence proportions of stage I, stage II, stage III, and stage IV patients were 5.88%, 27.05%, 52.35%, and 14.705%, respectively. Conclusion: Finally, the findings of this study implied that age, smoking cigarettes, stage of disease, initial treatment patients took, types of treatment patients took, and place were major factors related to the recurrence time of cervical cancer patients.
| Published in | Biomedical Statistics and Informatics (Volume 9, Issue 1) |
| DOI | 10.11648/j.bsi.20240901.12 |
| Page(s) | 9-21 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Survival Analysis, Proportional Hazard, Cervical Cancer, Recurrence Time
Variables | Description | Values |
|---|---|---|
Age | Age of the patients | or >50 |
Marriage | Age at Marriage | |
Chemotherapy | Cycles of Chemotherapy | No chemotherapy, 1st cycle and 2nd cycle |
Treatment | Treatment taken | Surgery, chemotherapy, radiotherapy, chemo-radiation, surgery and chemotherapy, surgery and radiotherapy |
Radiotherapy | Aim of radiotherapy | No RT, Palliative and radical |
Sexual | Sexual partner | One, two, few (2-3), multiple (>3) and unknown |
HIV | Status | No or Yes |
Abortion | No or Yes | |
Family | Family planning | No or Yes |
Family2 | Family history | No or Yes |
smoking | Smoking status | No or Yes |
Children | Number of children | No child, 1-3, 4-7 and 8 and above |
Stage | Stage of cervical cancer | Stage I, II, III, and IV respectively. |
Initial treatment | Surgery, chemotherapy, radiotherapy and combination. | |
Birth | Age at first birth |
|
Tumor | Tumor size (cm) | |
Tumor2 | Tumor grade | Well, moderate and poor |
Place | Place of origin | Urban/rural |
Covariate | Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
Β | Unadjusted HR | p-value | 95% CI | Β | Adjusted HR | p-value | 95% CI | |
Age | 1.3971 | 4.0434 | 4.69e-14* | (2.812, 5.814) | 1.1728 | 3.2309 | 1.3e-09* | (2.21, 4.72) |
Smoking | 1.2979 | 3.6616 | 2.35e-14 * | (2.623, 5.111) | 0.6783 | 1.9705 | 0.0004* | (1.35, 2.86) |
Stage of disease | ||||||||
StageI | Ref. | |||||||
StageII | -.6191 | 0.5384 | 0.00404 * | (0.353,.8211) | -0.0794 | 0.9235 | 0.831 | (0.44, 1.91) |
StageIII | -.3198 | 0.7263 | 0.11730 | (0.4867, 1.08) | -0.0794 | 0.9236 | 0.8201 | (0.46, 1.83) |
StageIV | -1.124 | 0.3250 | 0.00167 * | (0.1612 0.65) | 0.84615 | 2.3306 | 0.0263* | (1.10, 4.92) |
Initial treat | ||||||||
Surgery | Ref | |||||||
Chemotherapy | -0.619 | 0.5384 | 0.00404 * | (0.3530, 0.82) | -0.6192 | 0.5383 | 0.0079* | (0.34, 0.85) |
Radiotherapy | -0.319 | 0.7263 | 0.11730 | (0.4867, 1.08) | -0.4164 | 0.6594 | 0.0508 | (0.43, 1.00) |
Comnbination | -1.124 | 0.3250 | 0.00167 * | (0.1612, 0.65) | -0.8191 | 0.4408 | 0.0260* | (0.21, 0.90) |
Types of treat | ||||||||
Surgery | Ref. | |||||||
Chemotherapy | -1.374 | 0.2529 | 0.00393 * | (0.0993, 0.64) | -0.8947 | 0.4087 | 0.0780 | (0.15, 1.10) |
Radiotherapy | -1.200 | 0.3011 | 8.04e-05 * | (0.1658, 0.54) | -0.7021 | 0.4955 | 0.0415* | (0.25, 0.97) |
Chemoradition | -1.431 | 0.2389 | 2.94e-05 * | (0.1220, 0.46) | -0.9217 | 0.3978 | 0.0148* | (0.18, 0.83) |
Surgery and chemoradiation | -0.739 | 0.4773 | 0.33328 | (0.1067,2.13) | -0.0102 | 0.9898 | 0.9895 | (0.21, 4.56) |
Surgery and radiotherapy | -1.008 | 0.3646 | 0.33312 | (0.0472, 2.81) | -0.6870 | 0.503 | 0.5181 | (0.06, 4.04) |
HIV status | ||||||||
Have HIV | Ref | |||||||
No HIV | 0.3288 | 1.3893 | 0.0434 * | (1.01, 1.911) | 0.1730 | 1.1888 | 0.3273 | (0.84, 1.68) |
Place | ||||||||
Urban | Ref. | |||||||
Rural | 0.4653 | 1.5925 | 0.00318 * | (1.169, 2.169) | 0.3427 | 1.4088 | 0.042* | (1.01, 1.96) |
likelihood ratio test | 129.6 | |||||||
AIC | 1676.602 | |||||||
rho | chisq | p | |
|---|---|---|---|
Age | 0.1543 | 4.8143 | 0.0282 |
Smoking | -0.0440 | 0.3866 | 0.5341 |
as.factor(stage)2 | 0.0278 | 0.1821 | 0.6696 |
as.factor(stage)3 | 0.0404 | 0.3700 | 0.5430 |
as.factor(stage)4 | 0.0153 | 0.0481 | 0.8263 |
as.factor(initial.treat)2 | -0.1102 | 2.4703 | 0.1160 |
as.factor(initial.treat)3 | -0.0691 | 0.8954 | 0.3440 |
as.factor(initial.treat)4 | -0.0208 | 0.0782 | 0.7798 |
as.factor(treat.take)2 | 0.0872 | 1.4718 | 0.2251 |
as.factor(treat.take)3 | 0.0121 | 0.0330 | 0.8560 |
as.factor(treat.take)4 | -0.0295 | 0.1944 | 0.6593 |
as.factor(treat.take)5 | 0.0677 | 0.7849 | 0.3756 |
as.factor(treat.take)6 | 0.0484 | 0.3935 | 0.5305 |
HIV.status | -0.0437 | 0.3696 | 0.5432 |
place | 0.0693 | 0.9276 | 0.3355 |
GLOBAL | NA | 15.2439 | 0.4340 |
ACS | American Cancer Society. |
AFT | Accelerated Failure Time |
AIC | Akaike Information Criterion |
AIDS | Ac uired Immune Deficiency Syndrome |
ANC | Antenatal Care |
CC | Cervical Cancer |
CSA | Central Statistical Agency |
DHS | Demographic and Health Survey |
DNA | Deoxyrebose Nucleic Acid |
ECA | Ethiopian Cancer Association |
HDI | Human Development Index |
HIV | Human Immune Virus |
HPV | Human Pappiloma Viruses |
NHS | National Health Service |
PH | Proportional Hazard |
PO | Proportional Odds |
TASH | Tikur Anbessa Specialized Hospital |
WHO | World Health Organization |
Covariate | Category | recurrent | censored | Total percent | p-value |
|---|---|---|---|---|---|
Age |
| 38 | 16 | 47.6% | 0.000 |
| 132 | 72 | 52.6% | ||
Smoking | Non-smoker | 120 | 242 | 86.2% | 0.000 |
Smoker | 50 | 16 | 13.8% | ||
Stage of disease | stageI | 10 | 128 | 6.2% | 0.000 |
StageII | 46 | 15 | 32.6% | ||
StageIII | 89 | 10 | 51.7% | ||
Stage IV | 25 | 214 | 9.5% | ||
Initial treatment | Surgery | 5 | 4 | 2.1% | 0.002 |
Chemotherapy | 3 | 10 | 3.1% | ||
Radiotherapy | 152 | 214 | 87.1% | ||
Chemo-radiation | 10 | 22 | 7.6% | ||
Number of cycles | No chemo | 90 | 144 | 55.7% | 0.912 |
First cycle | 54 | 73 | 30.0% | ||
Second cylce | 26 | 33 | 14.2% | ||
Aim of radiotherapy | No RT | 4 | 2 | 1.4% | 0.636 |
Palliative | 112 | 151 | 62.6% | ||
Radical | 17 | 97 | 36.0% | ||
Tumor size |
| 126 | 191 | 75.5% | 0.255 |
>4 | 44 | 59 | 24.5% | ||
Types of treatment | Surgery | 4 | 0 | 1.0% | 0.001 |
Chemotherapy | 2 | 3 | 1.2% | ||
Radiotherapy | 127 | 189 | 75.2% | ||
Chemo-radiation | 34 | 53 | 20.7% | ||
Surgery-chemotherapy | 2 | 10 | 0.7% | ||
Surgery-radiotherapy | 1 | 4 | 1.2% | ||
HIV status | no | 113 | 180 | 69.8% | 0.041 |
yes | 57 | 70 | 30.2% | ||
Place | Urban | 68 | 127 | 46.4% | 0.003 |
rural | 102 | 123 | 53.6% |
Mean | ||||
|---|---|---|---|---|
Age of patients | Estimate | Std.Error | 95% confidence interval | |
Lower Bound | Upper Bound | |||
Less than or equal to 50 | 22.363 | .526 | 21.329 | 23.397 |
Greater than 50 | 16.437 | .526 | 15.406 | 17.467 |
Stage of disease | ||||
Stage I | 16.344 | 1.619 | 13.172 | 19.517 |
Stage II | 20.007 | .709 | 18.620 | 21.395 |
Stage III | 19.612 | .535 | 18.563 | 20.662 |
Stage IV | 13.745 | 1.176 | 11.443 | 16.050 |
Smoking habit of patients | ||||
Non-smoker | 20.217 | .424 | 19.387 | 21.047 |
Smoker | 12.919 | .883 | 11.189 | 14.649 |
Initial treatment of patients took | ||||
Surgery | 16.351 | .932 | 14.534 | 18.178 |
Chemotherapy | 19.884 | .679 | 18.552 | 21.215 |
Radiotherapy | 18.591 | .655 | 17.307 | 19.215 |
Comnbination | 21.974 | 1.144 | 19.733 | 24.216 |
Number of cycles patients took | ||||
No chemo | 19.16 | .546 | 18.089 | 20.230 |
First cycles | 19.082 | .730 | 17.652 | 20.512 |
Second cycles | 18.539 | 1.117 | 16.35 | 20.729 |
Aim of radiotherapy | ||||
No RT | 19.400 | 3.276 | 12.979 | 25.821 |
Palliative | 18.839 | .504 | 17.851 | 19.828 |
Radical | 19.387 | .703 | 18.003 | 20.757 |
Tumor size of cervical cancer | ||||
Less than or equal to 4 | 19.282 | .466 | 18.368 | 20.195 |
Greater than 4 | 18162 | .822 | 16.551 | 19.773 |
Types of treatment patients took | ||||
Surgery | 11.929 | 2.010 | 7.989 | 15.868 |
Chemotherapy | 20.706 | 1.743 | 17.290 | 24.122 |
Radiotherapy | 19.052 | .483 | 18.105 | 19.999 |
Chemoradiation | 19.952 | .894 | 18.193 | 21.679 |
Surgery and chemotherapy | 16.667 | 5.004 | 6.859 | 26.474 |
Surgery and radiotherapy | 13.000 | .000 | 13.000 | 13.000 |
HIV status of patients | ||||
No | 19.567 | .471 | 18.646 | 20.493 |
Yes | 17.695 | .786 | 16.155 | 19.234 |
Place where patients come | ||||
Urban | 20.369 | .576 | 19.241 | 21.497 |
Rural | 17.87 | .557 | 18.962 | 18.962 |
| [1] | M. H. Forouzanfar et al., “Breast and cervical cancer in 187 countries between 1980 and 2010: A systematic analysis,” Lancet, vol. 378, no. 9801, pp. 1461–1484, Oct. 2011, |
| [2] | J. UNFPA, IPPF, WHO, PATH, UICC, “Comprehensive Cervical Cancer Prevention and Control: Program Guidance for Countries,” OPUS, vol. 2, no. 4, 2011. |
| [3] | A. Gedefaw, A. Astatkie, and G. A. Tessema, “The Prevalence of Precancerous Cervical Cancer Lesion among HIV-Infected Women in Southern Ethiopia: A Cross-Sectional Study,” PLoS One, vol. 8, no. 12, p. e84519, Dec. 2013, |
| [4] | A. Mandić et al., “Stage IB2 cervical cancer: brachytherapy followed by radical hysterectomy,” J. BUON, vol. 10, pp. 371–375, 2005. |
| [5] | N. G. Campos, “Cervical Cancer Prevention: Using Primary Data to Inform Decision-Making in Developed and Developing Country Contexts - ProQuest,” ProQuest. |
| [6] | E. A. Waktola, W. Mihret, and L. Bekele, “HPV and burden of cervical cancer in East Africa,” Gynecol. Oncol., vol. 99, no. 3 SUPPL., pp. S201–S202, Dec. 2005, |
| [7] | M. Abdel-Wahab et al., “Status of radiotherapy resources in Africa: An International Atomic Energy Agency analysis,” Lancet Oncol., vol. 14, no. 4, pp. e168–e175, Apr. 2013, |
| [8] | S. T. Memirie et al., “Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data,” J. Glob. Oncol., vol. 2018, no. 4, pp. 1–11, Mar. 2018, |
| [9] | R. J. T. Sekse, E. Gjengedal, and M. Råheim, “Living in a Changed Female Body After Gynecological Cancer,” Health Care Women Int., vol. 34, no. 1, pp. 14–33, Jan. 2013, |
| [10] | K. Limmer, G. LoBiondo-Wood, and J. Dains, “Predictors of Cervical Cancer Screening Adherence in the United States: A Systematic Review,” J. Adv. Pract. Oncol., vol. 5, no. 1, p. 31, Jan. 2014. |
| [11] | G. Braun et al., “Cancer in Africa: AORTIC 8th International Cancer Conference ‘Entering the 21st Century for Cancer Control in Africa’ 30.11.−2.12.2011,” Breast Care, vol. 7, no. 2, p. 177, Apr. 2012, |
| [12] | S. Wittet and V. Tsu, “Cervical cancer prevention and the Millennium Development Goals,” Bull. World Health Organ., vol. 86, no. 6, pp. 488–490, 2008, |
| [13] | V. Turan and K. Oktay, “Sexual and fertility adverse effects associated with chemotherapy treatment in women,” Expert Opin. Drug Saf., vol. 13, no. 6, pp. 775–783, 2014, |
| [14] | S. Poolkerd et al., “Phone: 0-1888-1390,” J Med Assoc Thai, vol. 89, no. 3, pp. 275–82, 2006. |
| [15] | M. D. Holmes et al., “Non-Communicable Diseases in Sub-Saharan Africa: The Case for Cohort Studies,” PLOS Med., vol. 7, no. 5, p. e1000244, May 2010, |
| [16] | S. Endale and J. Ethiopia, “Modeling Time-to-Death of Women with Cervical Cancer: A Case Study at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia,” 2016. |
APA Style
Ettisa, D. L. (2024). Identify Primary Risk Variables Influencing the Recurrence of Cervical Cancer in Patients, Using Non-Parametric Methods at Tikur Anbessa Specialized Hospital. Biomedical Statistics and Informatics, 9(1), 9-21. https://doi.org/10.11648/j.bsi.20240901.12
ACS Style
Ettisa, D. L. Identify Primary Risk Variables Influencing the Recurrence of Cervical Cancer in Patients, Using Non-Parametric Methods at Tikur Anbessa Specialized Hospital. Biomed. Stat. Inform. 2024, 9(1), 9-21. doi: 10.11648/j.bsi.20240901.12
AMA Style
Ettisa DL. Identify Primary Risk Variables Influencing the Recurrence of Cervical Cancer in Patients, Using Non-Parametric Methods at Tikur Anbessa Specialized Hospital. Biomed Stat Inform. 2024;9(1):9-21. doi: 10.11648/j.bsi.20240901.12
@article{10.11648/j.bsi.20240901.12,
author = {Demelash Lemmi Ettisa},
title = {Identify Primary Risk Variables Influencing the Recurrence of Cervical Cancer in Patients, Using Non-Parametric Methods at Tikur Anbessa Specialized Hospital
},
journal = {Biomedical Statistics and Informatics},
volume = {9},
number = {1},
pages = {9-21},
doi = {10.11648/j.bsi.20240901.12},
url = {https://doi.org/10.11648/j.bsi.20240901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.bsi.20240901.12},
abstract = {Background: This study aimed to identify the primary risk variables influencing the recurrence of cervical cancer in patients, at Tikur Anbessa Specialized Hospital. Cervical cancer deaths in Ethiopia reached 4,595, or 0.76% of total deaths. The age-adjusted death rate is 18.51 per 100,000 of the population in Ethiopia. Method: Among patients with cervical cancer, an institution-based retrospective follow-up research was conducted from January 2015 to March 2017 at TASH and is under follow-up. Out of a population of cervical cancer patients who were taking treatment in the hospital during that period, data on 420 patients is included in this study. Non-parametric methods, such as log-rank tests and the Kaplan-Meier method, were used to compare the rate of recurrence among the different explanatory variable categories. Results: After the medical cards of women were reviewed among those patients with cervical cancer, 170 (40.5%) were recurrent, and the remaining 250 (59.5%) were censored. Out of the total patients, 6.2% were at stage I, 32.6% were at stage II, 51.7% were at stage III, and 9.5% were at stage IV. The recurrence proportions of stage I, stage II, stage III, and stage IV patients were 5.88%, 27.05%, 52.35%, and 14.705%, respectively. Conclusion: Finally, the findings of this study implied that age, smoking cigarettes, stage of disease, initial treatment patients took, types of treatment patients took, and place were major factors related to the recurrence time of cervical cancer patients.
},
year = {2024}
}
TY - JOUR T1 - Identify Primary Risk Variables Influencing the Recurrence of Cervical Cancer in Patients, Using Non-Parametric Methods at Tikur Anbessa Specialized Hospital AU - Demelash Lemmi Ettisa Y1 - 2024/08/15 PY - 2024 N1 - https://doi.org/10.11648/j.bsi.20240901.12 DO - 10.11648/j.bsi.20240901.12 T2 - Biomedical Statistics and Informatics JF - Biomedical Statistics and Informatics JO - Biomedical Statistics and Informatics SP - 9 EP - 21 PB - Science Publishing Group SN - 2578-8728 UR - https://doi.org/10.11648/j.bsi.20240901.12 AB - Background: This study aimed to identify the primary risk variables influencing the recurrence of cervical cancer in patients, at Tikur Anbessa Specialized Hospital. Cervical cancer deaths in Ethiopia reached 4,595, or 0.76% of total deaths. The age-adjusted death rate is 18.51 per 100,000 of the population in Ethiopia. Method: Among patients with cervical cancer, an institution-based retrospective follow-up research was conducted from January 2015 to March 2017 at TASH and is under follow-up. Out of a population of cervical cancer patients who were taking treatment in the hospital during that period, data on 420 patients is included in this study. Non-parametric methods, such as log-rank tests and the Kaplan-Meier method, were used to compare the rate of recurrence among the different explanatory variable categories. Results: After the medical cards of women were reviewed among those patients with cervical cancer, 170 (40.5%) were recurrent, and the remaining 250 (59.5%) were censored. Out of the total patients, 6.2% were at stage I, 32.6% were at stage II, 51.7% were at stage III, and 9.5% were at stage IV. The recurrence proportions of stage I, stage II, stage III, and stage IV patients were 5.88%, 27.05%, 52.35%, and 14.705%, respectively. Conclusion: Finally, the findings of this study implied that age, smoking cigarettes, stage of disease, initial treatment patients took, types of treatment patients took, and place were major factors related to the recurrence time of cervical cancer patients. VL - 9 IS - 1 ER -
Department of Statistics, Samara University, Afar, Ethiopia
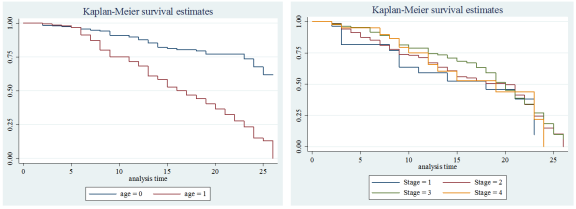
Figure 1. K-M survival time plot by age of cervical cancer patients.
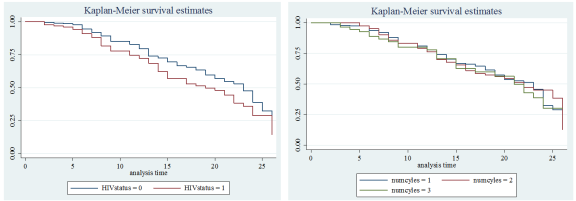
Figure 2. K-M survival time plot by HIV status and number of cycles of CC patients.
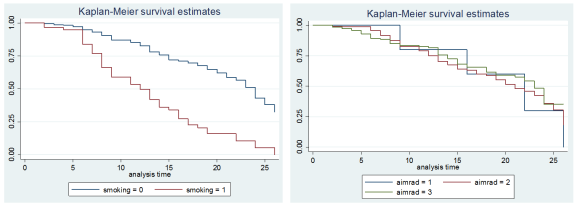
Figure 3. K-M survival time plot by smoking status and aim of the radiotherapy of CC patients.
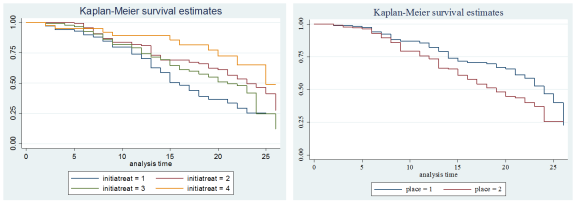
Figure 4. K-M survival time plot by initial treatment and place of CC patients.
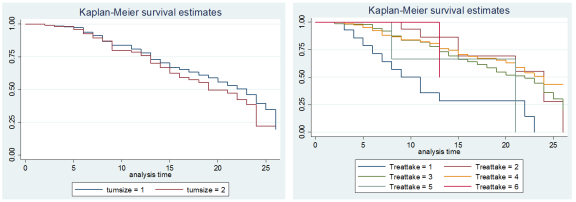
Figure 5. K-M survival time plot by tumor size and type of treatment taken of CC patients.

